ARGUMENTS TO MAKE TO SHOW MASK SCIENCE FICTION - PART 1
Feel free to use this article in court cases

There were two responses to the pandemic which consisted of a medical response and an exposure mitigation response. Many have inaccurately assumed that the medical industry has expertise in both areas but this is incorrect. The medical industry is unschooled in exposure science and is in fact a customer to the exposure science industry known as industrial hygiene. Medical scientists primarily work in an office whereas exposure control experts such as industrial hygienists operate in the field where workers and the public are located.
The medical response consists of learning about the pathogen in how it travels, how it affects and enters the body, the pathogen’s structure and weaknesses, and what treatments work after exposure to the pathogen has occurred. Exposure mitigation sciences will initially take the medical science, to specifically evaluate possible options for combating the pathogen. Then, each occupied space will be evaluated to identify current hazards and ensure a customized approach to each exposure will be met to ensure the occupants have optimal safety and health results.
The exposure science industry consists of occupational safety and health professionals and industrial hygienists. As such experts we work in concert to mitigate various exposures in every single industry. You will find us in construction, mining, manufacturing, law enforcement, the military, insurance, food service, government, consumer shopping, and yes we serve the medical industry too!
OSHA sums what industrial hygiene is as the “science and art devoted to the anticipation, recognition, evaluation, and control of those environmental factors or stresses arising in or from the workplace, which may cause sickness, impaired health and well-being, or significant discomfort among workers or among the citizens of the community.” While the American Industrial Hygiene Association (AIHA) defines an industrial hygienist as “scientists and engineers committed to protecting the health and safety of people in the workplace and the community.”
The Department of Labor defines a “qualified” person as one who by possession of a recognized degree, certificate, or professional standing, or who by extensive knowledge, training, and experience, has successfully demonstrated the ability to solve or resolve problems relating to the subject matter, the work, or the project. While we recognize the obvious significance that medical science is required for a competent pandemic response, we contend with the assumption that medical scientists are the qualified people to recommend exposure mitigation strategies.
History has shown this before but the public and media did not catch these past mistakes. An example of the inept training of control measures in the medical field occurred during the Ebola outbreak in 2014. A hospital in Dallas, Texas took in Ebola patients and found themselves completely unprepared. The medical professionals got on the internet and unprofessionally used some PPE and as a result nurses were exposed and became infected. Moreover, it can be assumed that the nurses were not fit tested for respirator use and no training on their control plan was provided. Thankfully, the nurses survived but the following link will show what was unveiled in court to the bungled measures taken (https://www.nbcnews.com/storyline/ebola-virus-outbreak/nurse-who-caught-ebola-settles-suit-against-dallas-hospital-n672081).
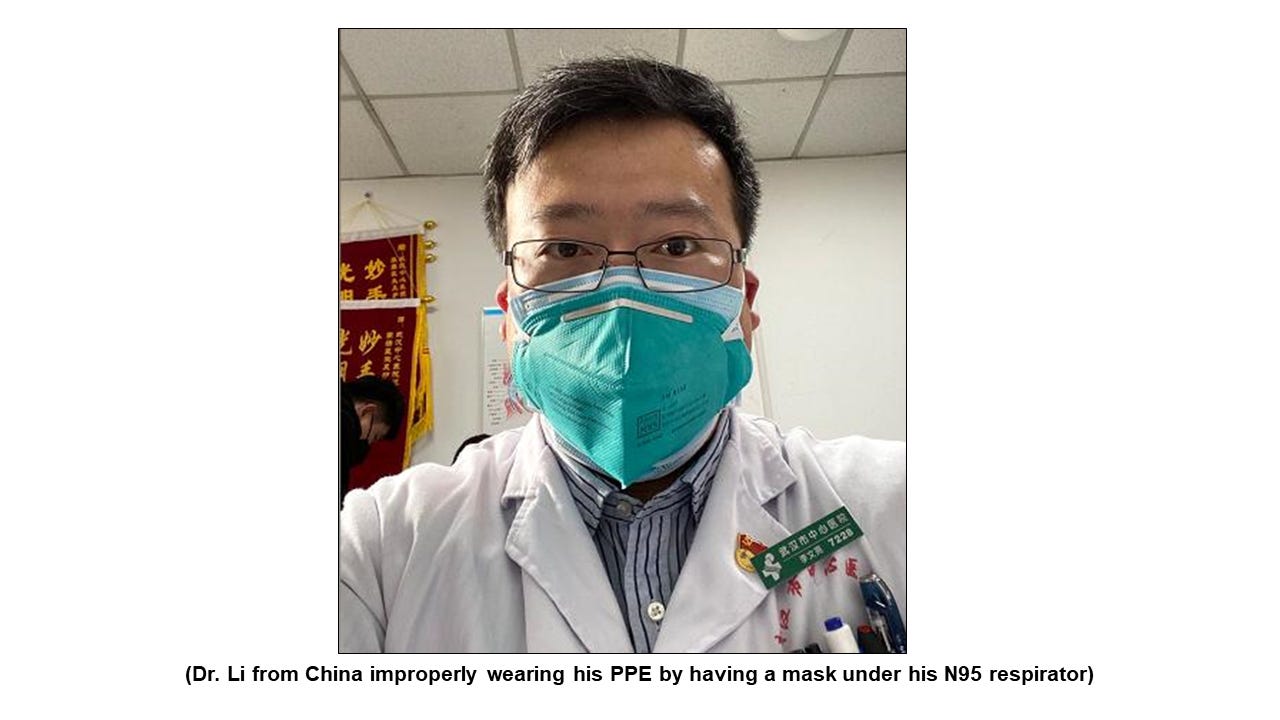
Even early in the current pandemic we witnessed firsthand the lack of training in the medical field on general PPE use. Petite nurses were wearing large disposable N95 respirators (clearly not fit tested), in some cases they took the bottom strap off, while others had their disposable N95 respirator on upside down. In addition, doctors were wearing a surgical mask with a disposable N95 respirator on top of it. This is improper use because the face mask was preventing the respirator from capturing a seal to the face.
There are pictures of the famous Chinese doctor (Dr. Li Wenliang) who warned the world of the current pandemic wearing his PPE in the same fashion as the before mentioned doctors. Unfortunately, Dr. Li’s improper use and choice of PPE was a likely contributing factor to his fatal exposure to the COVID-19 virus.
The inadequacies in the medical industry’s comprehension of exposure mitigation are further illustrated in that around 90% of the OSHA citations that involve the pandemic are in the medical industry. Their citations consistently revolve around violations of the regulatory standards in Personal Protective Equipment (PPE) (29 CFR § 1910.132) and Respiratory Protection (29 CFR § 1910.134). It is such a profound issue that OSHA is in the process of creating regulatory standards for the medical industry as it relates to COVID-19. We are scheduled to testify in that hearing on May 2, 2022. Now if the medical industry consisted of the qualified people for exposure mitigation the question that should be asked is why are they suffering from these significant shortcomings?
Some have contended with our position that school children and travel passengers do not fall under the Code of Federal Regulations (CFR) and our points are mute. This is inaccurate for two reasons; First, the N95 is in the forefront of the mask debate and it should be understood that the N95 is a respirator and not a mask. The “N” means the respirator is non-oil resistant and cannot be used in an environment where oil-based product exposures exist. The “95” means the filter has 95% efficiency which means it can only achieve that by being used correctly every single time. Further, it seals to the face which qualifies it as a respirator. As such, N95 manufacturers will require that the wearer should adhere to the Respiratory Protection standard for safe use.
Second, we are having people wear a mask because of safety and health concerns. So, the logical starting point should be to use established sciences related to the safety and health profession to build from. Therefore, it is important for professionals in our industry to be engaged in this debate to ensure the bar for safety and health sciences is not lowered by the unqualified. This “CFR” argument seems to be a convenient way to make over seventy years of safety and health sciences disappear on a “departmental jurisdiction technicality”.
We believe the court should end the mask mandate enforced by the TSA because there has never been scientific evidence that supports universal mask use, that air travel is already equipped to provide a safe experience, the use of PPE by untrained people creates more risk, and that mask guidance continues to come from unqualified scientists traveling outside of their lane of expertise. We have four primary reasons why this court should consider our position.
Reason #1: The mitigation strategy delivered by public health officials has not been prioritized in accordance with the Hierarchy of Controls.
We have been in several conversations with doctors and school administrators on COVID-19 exposure mitigation tactics and have been met with the straw man argument that nobody really knows which exposure control measures are working and which ones work better than others. In fact, these words even came from medical professionals that were tasked with developing and implementing such tactics in schools. These types of comments are an indicator of an unqualified scientist traveling outside of their scope of expertise.
As occupational safety and health professionals and industrial hygienists, we can affirm that our profession consists of trained experts in evaluating an environment for risks and exposure with the ability to measure the determined exposures and devise a mitigation plan. We use a long standing proven scientific system call the Hierarchy of Controls (Figure 1-A) that was introduced by the National Safety Council (NSC) in 1950 to layer our exposure mitigation strategies. This system also enables us to prioritize the mitigating efforts to better educate our customers as to which strategies are going to work the best.

The human interaction with a control, while it is engaged with the risk or contamination, is a primary difference between the class of controls on the high end of the hierarchy and those at the low end. In any compliance program, the most critical component of whether it will succeed or not is in fact human behavior. We see behavior being the cause of 90% of roadway collisions, cyber-attacks, and workplace incidents. Human behavior as it relates to compliance or safety and health, is such juggernaut that we have entire education courses on Behavioral Based Safety, which is why we always seek solutions that have a foundation in engineering controls.
Engineering controls isolate people from the hazard while the design and function of an administrative control is maintained by specific consistent proper execution of the procedural control. Any deviation from that then becomes contamination behavior and is deteriorating or downgrading its effectiveness. Then at the bottom of the effectiveness chain is the PPE category of controls. With PPE there is complete reliance on human use and interaction, to maintain its designed scope of protection. In our careers we have experienced personnel failing to use their PPE due to a lack of comfort, poor training, or myths they carried with them from a previous employer.
Masks do not seal to the face and cannot offer protection. It can reduce exposure to blood splatter for medical professionals at best, but it is not deemed a true protective piece. Therefore, a mask can in no way scientifically be considered a primary solution to an exposure issue as many doctors and politicians have claimed. A competent response would be focused on dilution, filtration, and destruction of the pathogen that are found within engineering controls.
Thankfully, air travel provides a state-of-the-art ventilation system that provides fresh air to the cabin typically every six minutes and pushes the air in a laminar motion to reduce cross contamination. This is important to understand because the AIHA conducted a study in 2020 (Figure 1-B) that found engineering controls (such as a ventilation system) provide the optimal solution for human protection. They produced a graph demonstrating a 95-99.9% risk reduction for exposure by simply having six to twelve air changes per hour.
It should be noted that this study was done in a medical setting with trained personnel in hygiene, sanitization, donning and doffing. The N95’s optimal performance is based on the user’s adherence to the Respiratory Protection standard as well as the manufacturer’s requirements for discarding the N95 after two to four hours of use.

By having an educated understanding in the fundamentals in exposure sciences, it is clearly seen that the solution has always been through engineering controls. However, early in the mask debate unqualified scientists conducted studies that promoted mask use but had there been an understanding in the hierarchy of controls, this confusion could have been averted.
For example, the “Absence of Apparent Transmission of SARS-CoV-2 from Two Stylists After Exposure at a Hair Salon with a Universal Face Covering Policy in Springfield, Missouri, May 2020” study has been a foundational piece used by public health to make the false claim that face masks are an added value when deployed in a community. We investigated this study, and a full report can be provided upon request. Here is an overview of our findings:
The study insinuates that one hundred and thirty-nine clients were not infected but the researchers in fact cannot make that claim. The sample size was one hundred and thirty-nine, but the researchers were only able to collect factual evidence on sixty-seven clients. Thirty-seven clients who were contacted refused to be tested and were self-reporting during a period when people had an incentive not to report themselves being sick, due to quarantine and isolation expectations. Another thirty-five clients were not contacted and did not receive a test, nor did they participate in self reporting. The fact of the research is that only 48% of the sample size was factually evaluated, while 52% had no factual data.
They study admitted limitations in administrative controls of limiting services and stylists and clients not facing each other during services. Administrative controls enable personnel to work or operate with a heightened level of safety and all such controls are considered a higher form of control than PPE. By not facing one another, clients and hair stylists made their experience significantly safe by making the flow of transmission that much more difficult. This was a significantly missed opportunity by the research team to demonstrate multiple measures people can take to prevent transmission. This should have been properly assessed and quantified in the study. This may be evidence of a bias of the research team in attempting to demonstrate the need for mask use. Regardless, by not properly evaluating all forms of controls in accordance with the well-established hierarchy demonstrates a significant lack of knowledge of this subject matter and those involved are unable to properly evaluate such event.
The study did not admit limitations by not evaluating sanitization efforts. The sanitation of surfaces is a combination of administrative and engineering controls. These are administrative controls because of the consistent processes for surface cleaning efforts. They are also engineering controls because the cleaning agents utilized end the flow of contamination. These are higher forms of controls in mitigating the risk of exposure. By not properly evaluating all forms of controls in accordance with the well-established hierarchy demonstrates a significant lack of knowledge of this subject matter and those involved are unable to properly evaluate such event.
The study did not admit the limitation of not evaluating the HVAC system. By having an active HVAC system airborne aerosol that carry infectious disease will be mitigated from the occupied space and prevent other personnel from being exposed. Other than eliminating the hazard the HVAC system is the first line of defense and the most critical exposure prevention method in a building. A focused emphasis should have been placed on evaluating this critical defense mechanism. By not properly evaluating all forms of controls in accordance with the well-established hierarchy demonstrates a significant lack of knowledge of this subject matter and those involved are unable to properly evaluate such event.
It is clearly seen in this study that it is not what would be considered evidence-based science that should drive public health policy, but it is still a foundational study used by public health officials around the world to push universal masking.
Thank you for your very informative articles , I'm still dumbfounded that professionals that should know better are still demanding masks be worn.
What is most disconcerting is the fact that foundational science was completely obliterated by the nonsense that insists you listen to it, with memes "Follow the science"
It's an utter mind F**k