
HOW MASKS WORK – THE MISSING PIECE
HOW MASKS WORK – THE MISSING PIECE
The critical aspect of a successful PPE program that nobody is discussing

Masks really are not doing what public health officials claim they are doing, and likely never were. Here's the important part of this missing piece and it has little to do with the fabric, the filters, or the tightness. The one thing that has not been explored in the COVID-19 science literature is how the mask interfaces with the short comings of human behavior.
In any compliance program, the most critical component of whether it will succeed or not is in fact human behavior. We see behavior being the cause of 90% of roadway collisions, cyber-attacks, and workplace incidents. Human behavior as it relates to compliance or safety and health, is such a juggernaut that we have entire education courses on Behavioral Based Safety.
Since getting into this industry, behavioral safety has constantly been discussed and programs have been developed to counter this significant barrier to a successful Environmental, Health, and Safety (EHS) Program.
The Safety Triangle is also known as the Heinrich or Safety Pyramid, is an idea that depicts a constant ratio amongst human behaviors that turn into workplace events of varying levels of severity.

The safety pyramid concept has contrasting opinions to it but has been a foundational component in the development of EHS programs through the 20th century. The point I’m making with it, is that countering the pit falls of human behavior as it relates to a successful EHS program has been a critical priority for decades.
To counter the shortcomings of human behavior, I have adopted several key elements to each EHS program that I have managed over the past decade.
Monitor and Measure: Key Performance Indicators (KPI’s) are critical to monitor and measure you program to identify successes and failures. By having this critical component adjustments can be made to the EHS program’s strategy if failures are occurring.
Audits and Inspections: These are components of any KPI strategy and when done properly will provide clarity to organizational expectations. These procedures define how to audit/inspect, what schedules to follow, and how to retain these records.
Targets and Objectives: Every fiscal or calendar year a healthy EHS program will identify tangible goals to achieve and a means in which those goals will be met. KPI’s will enable EHS program administrators to adjust measures to fulfill set targets.
Communication: Communication can come in the form of meetings, letters, emails, and phone calls. Organizations are best served when procedures on methods and retention of internal and external communications are established.
Document Control: Organizations will typically get littered with forms and other documents with no order in understanding which ones are expired or many will be redundant. The document control process will enable an organization on how to develop and use controlled documents.
Record Retention: Once a document is used for something like an inspection, it becomes a record. Compliance records carry significant weight in managing an EHS program and it is critical to have them organized and scheduled for a specific retention period.
Legal Requirements: Identifying all the legal aspects of your program to understand countermeasures to put in place.
Change Management: When organizations experience promotions, terminations, job transfers, growth, or a decrease in staff, critical aspects to the business can be lost or fall through the cracks in these types of transitions. Management of Change is a key process that attempts to lay out a safety net to catch as many of these concerns as possible.
Risk Identification: The inability to identify risks is a top three reason for safety failures. When establishing a functional EHS program going into each aspect of the business to identify risks is vital to implementing proper exposure prevention methodologies. A one size fits all approach is a recipe for failure and identifying the specific nature of each department will unveil their risks. Safety Plans or a Job Hazard Analysis are examples of such measures.
Training: A comprehensive training program that covers all aspects of exposure prevention measures and the expectations of personnel is paramount to providing clarity. Such a training program will encompass initial, weekly, quarterly, annual, and post incident training.
By having these key elements an EHS program can be governed by three key principles of being Proactive, providing Clarity, and achieving Buy-In from the top down of the organization.

After two years of Federal Government buffoonery, how much better would the state of our country or world be had EHS professionals been involved in the creation and direction of the Safety and Health program for the COVID-19 response? Was the government Proactive? Did they ever provide Clarity? In my professional opinion, governments around the world failed in these two principles which is why they have not achieved Buy-In from a significant portion of the world’s population.
A QUICK REFRESHER IN EXPOSURE SCIENCE
I want to shed some light on a critical aspect of PPE that is often overlooked, misunderstood, or just ignored by people who demand mask mandates. Universal masking mandates have had this key mechanism of countering behavioral short comings removed which deals with contamination, but medical facilities still have this piece attached to their masking protocols.
The human interaction with a control, while it is engaged with the hazard or contamination, is a primary difference between the class of controls on the high end of the hierarchy and those at the low end.
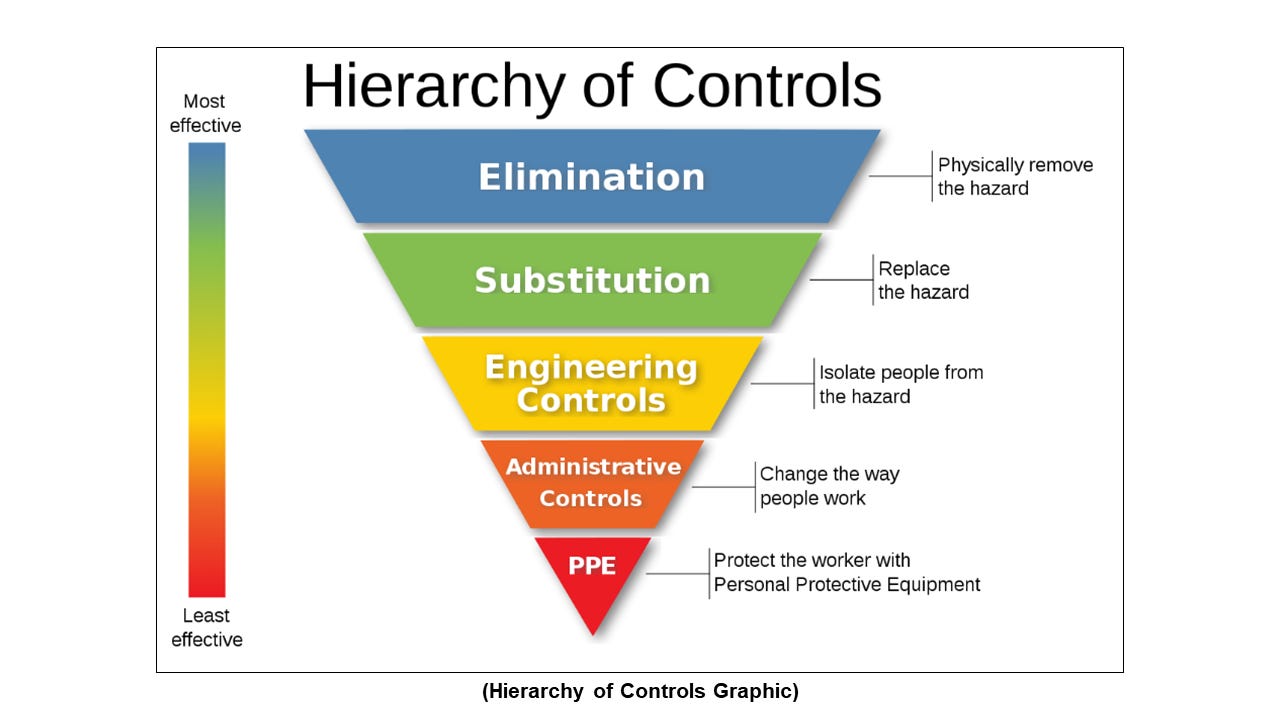
Engineering Controls isolate people from the hazard while the design and function of an Administrative Control is maintained by specific consistent proper execution of the procedural control. Any deviation from that then becomes contamination behavior and is deteriorating or downgrading its effectiveness. Then at the bottom of the effectiveness chain is the PPE category of controls. With PPE there is complete reliance on human use and interaction, to maintain it's designed scope of protection.
How the tool is used determines how well the PPE’s engineering can achieve what it is designed to accomplish. This is true for any tool. Let’s say, you sit down to eat cereal or soup and you have the world’s best designed spoon. Great, but put that spoon in your mouth upside down and you've instantly eliminated the capability of its design and engineering from coming into play.
Conversely, An HVAC or UV-C system, as contamination control, doesn't require continual human interaction while it is doing what its designed to do. You turn on a switch and the engineering of it alone are the bulk of the contamination protection process. Yes, it still requires human interaction at certain points, for maintenance and assembly, but then the human involvement is removed for the bulk of time the control interfaces with the hazard.
The same as a light bulb which doesn't require constant human monitoring, or effort to keep the brightness shining, while it lights a room. With PPE, human control is present during the entire time the PPE is interfacing with the hazard. More importantly the human is in direct contact with the risk or hazard the entire time. Read that again…the human is in direct contact with the risk or hazard the entire time.
Human interactions or requirements that have less constant involvement with the protection mechanisms, the further up the Hierarchy of Controls you go. PPE has been deployed as if it were an Engineering Control or an automated machine. Just put it on the face and it just automatically does its thing. This is the thinking of people who only have a limited perspective of the sciences that are in play.
Let me ask you something important. Does the water or spittle material itself cause infection, or is it the virus material that causes infection? The virus material causes infection, therefore, that is the only part of the equation that matters. Where it goes and what's happening to it is ultimately is what we need to know.
Every mask experiment on the CDC’s website only shows how water droplets land in a mask. Then the experiments stop. There is no exploration of where the infectious material goes next. If you have a mask on your face for several hours in a day, that's a lot of time and opportunity for contamination to go somewhere next.
Let me put it another way. That's several hours of you the human, being in direct contact with the contaminates (hazards) while you go about your day interacting with surfaces and other people. Oh, and I'm pretty sure you never once washed your face at school or work between masks. That's just one of many ways you've been helping contamination to go somewhere next.
Every mask case study on the CDC's website is predicated on the notion that masks are an Engineering Control. When they are placed on the face then they are working at 100% optimal levels. Like turning the power switch on. Case studies look at spreadsheet data that says whether masks were on faces or not, and during which times and not. No case study has ever calculated the contamination behavior taking place that is continually working to negate, what was already, at best, a minimal measurement of protection.
What happens to your case study when the tool you are measuring isn't being used correctly? To put it bluntly, it means that tool likely isn't the thing producing the supposed data. The real numbers are somewhere much lower, maybe even zero, or have become a negative and the effort is generating pure risk.
In following the Hierarchy of Controls other mitigation factors in these case studies had more impact in reducing infections than the piece of germ contaminated cloth on the face did.
Examples of these other factors are Administrative Controls such as healthy habits, taking vitamins, personal hygiene, sanitization protocols that use cleaners, public distancing; or Engineering Controls such as individual immunity, HVAC, and UV-C systems; or operating remotely and Eliminating risks at work were all in play with mask mandates.
PPE IS NOT A LIGHT BULB, IT’S A SPOON
As before described, erroneous human behavior is the biggest reason for systems breaking across all industries. Not just in safety and health. Human error is the biggest and most consistent reason why things don't work right.
In the medical industry doctor error has been a top ten leading cause of death for decades. Even new industries like cyber security where optimal technology is utilized, still human mistakes are the leading cause of security system failures. Now, with the issue of universal public masking, at least 90% of public mask behavior is contamination behavior, continually negating the ability for any mask or respirator from preventing contamination and exposure.
When PPE is used in the professional environment it was designed for, it is legally required (29 CFR § 1910.132(f)) to be accompanied by strict behavioral processes for the purpose of reducing contamination behavior. That's what it takes for a mask to succeed in its role. This critical mechanism of mask functionality has been entirely removed in the public use of masks and respirators.
Why did the mask using doctors, who are prescribing public deployment of masks think masks would somehow magically work without compensating for contamination behavior? If we are going to be scientifically consistent, we must be able to reproduce this in all settings.
Should we have all hospitals stop the donning and doffing of their goggles, gowns, gloves, respirators, and masks? Because the message from doctors influencing public policy is clearly that behavior is not important to the protective function of a mask or respirator. That goes against everything we are taught and execute in the Industrial Hygiene and Risk Management profession.
Which begs the question about donning and doffing procedures, since for two years now, doctors believe that masks aren't contaminated, why then are hospitals still engaged in this superstitious ritualistic waste of time? That was sarcasm…in case you couldn’t tell.
There is something else that is important to distinguish.
Authorities, doctors, and scientists have somehow equated giving us instructions or reminders about mask use, to be the same thing as assuming it occurs in the real world. You see comments much like this from people in authority...
“A mask should still provide some protection in an unmasked setting, assuming it's well fitted and worn correctly, and you don't continually adjust or touch it”.
Ok that's fine...but what about when it’s not worn correctly or tightly fitted, or not touched or adjusted? What happens then? This is an important question don't you think?
THE DO’s AND DON’Ts
A mask’s ability to work properly is presumptive upon being worn properly, fit tightly, not touched, not adjusted, and cleaned, therefore if it is not properly worn, fitted, cleaned, or touched, it is NOT fulfilling its role. Public health officials and TV doctors have failed to address this issue.
I have some questions for the CDC and the WHO. Why did you put these things on this list of DON’Ts.? In other words, how did you determine that these behaviors should belong on the “DON’T” list?
Secondly, what will happen if somebody DOES do the DON’Ts?

This is probably an important question to explore on behalf of every consistent mask wearer on the planet. Is this potentially rendering the net benefit of masks to zero or even worse by creating pure risk?
Since the CDC doesn't want to address it, I'll take a crack at it…
This is what happens when you DO the DON'Ts:
You create more exposure points and risks.
You enable the trail of contamination to make its next step.
You significantly reduce and potentially nullify any protection or spread prevention the mask is trying to accomplish for you.
Or to put it another way...if you don’t correlate proper behavior with the deployment of masking (just as with any PPE policy) the mask doesn’t work and causes harm!
Masks aren't doing what the media and TV doctors say they are doing, and they never were.
I work in a greenhouse and we grow perennial liners.
Although wide scale pesticide spraying is minimal due to pest control using biologicals.
Prior to the use of bio's we used a big yellow tank which holds 100's of gallons of pesticide mix and gets sprayed out via a gun that creates fine mist which gives excellent penetration.
The mist spray particles from the gun is far more larger than that of a aerosolized virus and yet I would never attempt using this equipment without are REAL Respirator with cartridges along with full donning of PPE suit head to toe.
What is extremely frightening is the science being flaunted by so called professionals is complete garbage ..
Psychological gas lighting.
Very disturbing