
THE PUBLIC NEEDS TO LEARN THE HIERARCHY OF CONTROLS
THE PUBLIC NEEDS TO LEARN THE HIERARCHY OF CONTROLS
AND WHY WE NEED TO STOP TALKING ABOUT PPE AS A REAL SOLUTION

The COVID-19 Pandemic response has been a complete disaster, and frankly that’s being kind. I know many will agree with my opinion and some will not understand my criticism of the response. In this article I will explain why I believe this response has been terrible and give some insight into why the response was a failure, but also give some hope for all of you in making good scientific decisions going forward during this pandemic and future ones.
WHAT IS EXPOSURE SCIENCE?
We had two responses to the pandemic which consisted of a medical response and an exposure mitigation response. The medical response consisted of learning about the pathogen, how it affects the body, how it enters the body, and what treatments work after exposure to the pathogen has occurred. The exposure mitigation first takes the medical science, to specifically know how the pathogen travels, enters the body, and what its composition is like to better understand its weaknesses.
Many have falsely assumed that the medical industry should handle both angles in this response but this is incorrect. The medical industry is unschooled in exposure science and is in fact a customer to the exposure science industry.
The exposure science industry consists of Occupational Safety and Health Professionals and Industrial Hygienists. These experts work in concert to mitigate various exposures in every single industry. Yes, there’s an entire industry that does nothing but mitigate exposures in every field of work. You will find us in construction, mining, manufacturing, law enforcement, the military, insurance, food service, government, consumer shopping, and yes we serve the medical industry too!
I think OSHA sums what Industrial Hygiene is best… “that science and art devoted to the anticipation, recognition, evaluation, and control of those environmental factors or stresses arising in or from the workplace, which may cause sickness, impaired health and well-being, or significant discomfort among workers or among the citizens of the community.”
As an Occupational Safety and Health Professional and Industrial Hygienist, I can affirm that my profession consists of trained experts in evaluating an environment for risks and exposure with the ability to measure the determined exposures and devise a mitigation plan. We use a long standing proven scientific system call the Hierarchy of Controls to layer our exposure mitigation plans. This system also enables us to prioritize the mitigating efforts to better educate our customers as to which strategies are going to work the best.
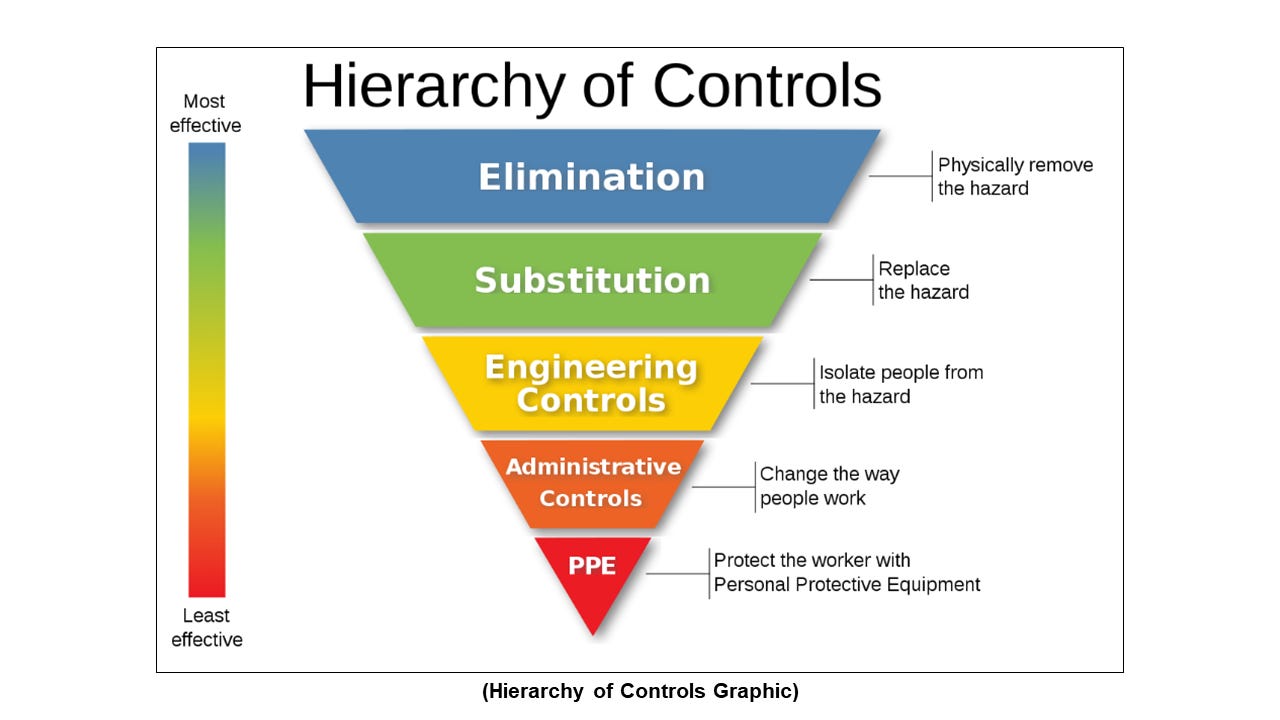
The Hierarchy of Controls is a system used to implement effective controls within an organization, workplace, or community to identify the most effective ways to mitigate hazards. Within the inverted pyramid below the more effective controls are on the large, top side of the pyramid, whereas the least effective controls are on the bottom. Following this hierarchy normally leads to the implementation of inherently safer systems, where the risk of illness or injury has been substantially reduced. Here is a brief description of each level of effectiveness – from most effective to least effective – within the Hierarchy of Controls model.
Elimination Controls
Elimination is a hazard control strategy based on completely removing a material or process causing a hazard. Elimination is the most effective of the five members of the hierarchy of controls in protecting personnel, and where possible should be implemented before all other control methods.
Removing the use of a hazardous chemical is an example of elimination. Some substances are difficult or impossible to eliminate because they have unique properties necessary to the process, but it may be possible to instead substitute less hazardous versions of the substance. Elimination also applies to equipment as well. For example, noisy equipment can be removed from a room used for other purposes, or an unnecessary blade can be removed from a machine.
Substitution Controls
Substitution is a hazard control strategy in which a material or process is replaced with another that is less hazardous. Substitution is the second most effective of the five members of the hierarchy of hazard controls in protecting people, after elimination.
A common substitution is to replace a toxic chemical with a less toxic one. Some examples include replacing the solvent benzene, a carcinogen, with toluene; switching from organic solvents to water-based detergents; and replacing paints containing lead with those containing non-leaded pigments.
Engineering Controls
Engineering controls is the third of five members of the hierarchy of controls, which orders control strategies by their feasibility and effectiveness. These are strategies designed to protect workers from hazardous conditions by placing a barrier between the person and the hazard or by removing a hazardous substance through air ventilation. Some examples of engineering controls are Heating, Ventilation, and Air Condition (HVAC) systems, area specific air ventilation systems, Ultraviolet (UV) air sanitation systems, specifically designed workspaces, machine guards, and physical barriers.
Administrative Controls
Administrative controls are the efforts to change the behavior of personnel to act safer. Within organizations, this is typically done through training, policies, procedures, and disciplinary action. Generally, administrative controls are cheaper to begin, but they may become more expensive over time as higher failure rates and the need for constant training or re-certification eclipse the initial investments of the three (3) more desirable hazard controls in the hierarchy.
Personal Protective Equipment
The purpose of personal protective equipment (PPE) is to reduce human exposure to hazards when engineering controls and administrative controls are not feasible or effective to reduce these risks to acceptable levels. PPE is needed when there are hazards present and is regarded as the last line of defense. PPE has the serious limitation that it does not eliminate the hazard at the source and may result in personnel being exposed to the hazard if the equipment fails or is misused.
Examples of PPE use is protective clothing, helmets, eye and hand protection, or other garments or equipment designed to protect the wearer’s body from injury or infection. The hazards addressed by such protective equipment include physical, electrical, heat, chemicals, biohazards, and airborne particulate matter.
This is the least effective control due to the extreme dependency on the human element. The PPE failing is always a concern, but human error occurs often with its use. In my career I have experienced personnel failing to use their PPE due to a lack of comfort, poor training, or myths they carried with them from a previous employer.
A former co-worker once believed that he could wear a respirator with a beard. He was never challenged by previous employers on this thought and worked over 30 years with misusing his respiratory protection while engaged in work activities that required the use of carcinogenic chemicals. When our paths met, I informed him that his form of respiratory protection required him to be clean shaven, I showed him in the standard, and did eventually sway him in the right direction.
It was a memorable experience because he tried to convince me I was wrong with showing me how Liam Neeson wore a respirator with facial hair in a Batman movie. I love Batman but when he showed me this scene from the movie, I truthfully could not help myself from giving him a rough time. Calling him “The Batman” eventually became a fun inside joke between he and I! Unfortunately, I recently learned that he was diagnosed with lymphoma and is fulfilling therapy in hopes of recovery. He was in his early sixties when diagnosed and the doctor did affirm to him that his workplace exposure was the likely culprit.
In terms of where a face mask fits in the Hierarchy of Controls…well, it really does not. Masks do not seal to your face and thus cannot protect you. It can reduce exposure to blood splatter for medical professionals at best, but it is not deemed a true protective piece. Therefore, a mask can in no way scientifically be considered a primary solution to an exposure issue as many doctors and politicians have claimed. A competent response would be focused on dilution, filtration, and destruction of the pathogen that are found with Engineering Controls.
WHY WAS THE EXPOSURE MITIGATION RESPONSE A FAILURE?
The short answer as to why our mitigation response was such a failure is that we had scientists giving recommendations to a lane of science they’re not schooled in. For example, they read these mask studies and assumed that those scientists did their job correctly. Because they are unschooled in exposure sciences, they were unable to understand proper methodologies of conducting mask tests and failed to recognize that the studies they were using were all flawed. Those mask tests coincidently were conducted by engineers and scientists who were also unschooled in exposure sciences. So, it has been layers of incompetency that has been leading this disaster.
History has shown this before but the public and media did not catch these past mistakes. An example of the inept training of control measures in the medical field occurred during the Ebola outbreak in 2014. A hospital in Dallas, Texas took in Ebola patients in and found themselves completely unprepared. The medical professionals got on the internet and threw some PPE together and when nurses were exposed, they became infected. They were using improper PPE, likely not fit tested for respirator use, and had no training on their control plan. Thankfully, the nurses survived but the following link will show what was unveiled in court to the bungled measures taken (https://www.nbcnews.com/storyline/ebola-virus-outbreak/nurse-who-caught-ebola-settles-suit-against-dallas-hospital-n672081).
The medical industry receives training on PPE to use in their settings but is not extensively trained in the Hierarchy of Controls and how to strategically use them in various settings. Soon after the pandemic began, I visited my doctor and I witnessed firsthand the lack of training in the medical office on general PPE use. Petite nurses were wearing large disposable N95 respirators (clearly not fit tested), in some cases they took the bottom strap off. I even helped a nurse become aware that her disposable N95 respirator was upside down. In addition, my doctor was wearing a surgical mask with a disposable N95 respirator on top of it. This is improper use because the face mask was preventing the respirator from capturing a seal to his face.
There are pictures of the famous Chinese doctor (Dr. Li Wenliang) who warned the world of this virus wearing his PPE in the same fashion as my doctor. Unfortunately, Dr. Li’s improper use and choice of PPE was a likely contributing factor to his fatal exposure to the COVID-19 virus.

I have been in settings that led to debates with medical professionals on exposure control strategies and most of them were convinced that masks work and that PPE is our first line of defense. Yes, I have had doctors actually tell me that PPE is the first line of defense! My next question to them is, “have you ever heard of the Hierarchy of Controls”? Every time I have asked that question to a medical professional, the answer is always…no. So, without that foundation, how in the world can you competently strategize an exposure mitigation plan? The answer is you cannot!
Many doctors across the world have fraudulently put themselves in the driver’s seat, claiming to have expertise in this subject matter to implement these strategies in businesses, schools, and communities. I experienced this firsthand in the city of Twin Falls, Idaho back during the winter of 2020. The town leaders were considering implementing a mask mandate at the demands of the local hospital system. They had a quack doctor go into the media and use garbage mask studies for justification. However, this doctor had no clue about the exposure science field, did not have the training to decipher the mask studies being used, and pushed a nonsensical argument for a town mask mandate. - See my Mask Documentary series as a reference to the garbage mask studies https://www.tyscienceguy.com/mask-documentary-series.html
I have family that lives in Twin Falls and a family member put me in touch with some of the local leaders that were opposed to the proposed mandate. I participated in a couple of interviews, a town rally, and thankfully the town’s leaders tabled the proposal, and the issue has not come back since.
The medical professionals that have called themselves experts in exposure mitigation are all responsible for this failure! Their fraud has confused the public, provided improper directives, hurt and in many cases destroyed businesses for no reason, and more importantly put people in harm’s way. My advice, keep track of those quacks in your community who have pushed this PPE nonsense and stop giving them your business.
WHAT HAVE BEEN THE CONSEQUENCES OF THE WRONG SCIENTISTS BEING IN CHARGE?
Imagine if we learned during the summer of 2020 that the COVID-19 illness had the potential to kill 25% of our children. What would you do? What would schools do? What would the media and politicians say? Well, I can tell you as a parent, I would do everything possible to protect my child from this exposure. Did anyone from school boards, the media, or any politicians demand exposure preventative measures when we learned from the CDC in the summer of 2020 that 25% of children were considering or had already committed harm to themselves because of the COVID-19 response measures? No, they all did nothing to protect children from this more harmful exposure created by THEM!
The doctors and teacher’s unions pushed for masking and isolating kids for no reason. We learned early in the pandemic that children were not being harmed by the virus and in fact had a higher chance of harm from the seasonal flu. We also had data showing that children were not spreading the disease either. So even if masks worked, why would you take these measures on children when the data showed it was unnecessary? Why would you double down on these measures when you learned early that is was created an exposure that could negatively harm 25% of kids?
Due to the limitations of medical scientists not understanding exposure science, they suffered from tunnel vision and created a more harmful exposure for children than the COVID-19 virus. It is mind-blowing to me to see people who still think this is science based and good for children. Anyone that still supports these measures must take a look at themselves from a moral perspective.
There are other known risk factors that have been blatantly been disregarded such as hypoxia and contamination. However, during this pandemic we are sadly learning that severe phycological issues are occurring as a result of daily mask use. We need scientists in the medical profession to start being honest about their competencies and limitations, instead of exercising their hubris into seeing themselves as the end all be all in every form of science.
WHAT CAN WE DO GOING FORWARD AND IN FUTURE PANDEMICS?
So, what do we do now? We have to first acknowledge that we were lied to and misled by those who did not have the qualifications and capabilities to properly lead an exposure response. Then the public must be trained on the Hierarchy of Controls and have a better foundation to exposure solutions. The American Industrial Hygiene Association (AIHA) published the Reducing the Risk of COVID-19 Using Engineering Controls guidance document in September of 2020. They produced a graph demonstrating a 95%-99.9% risk reduction for exposure by simply having six to twelve air changes per hour. The CDC and other Public Health officials never acknowledged this measure…ever!
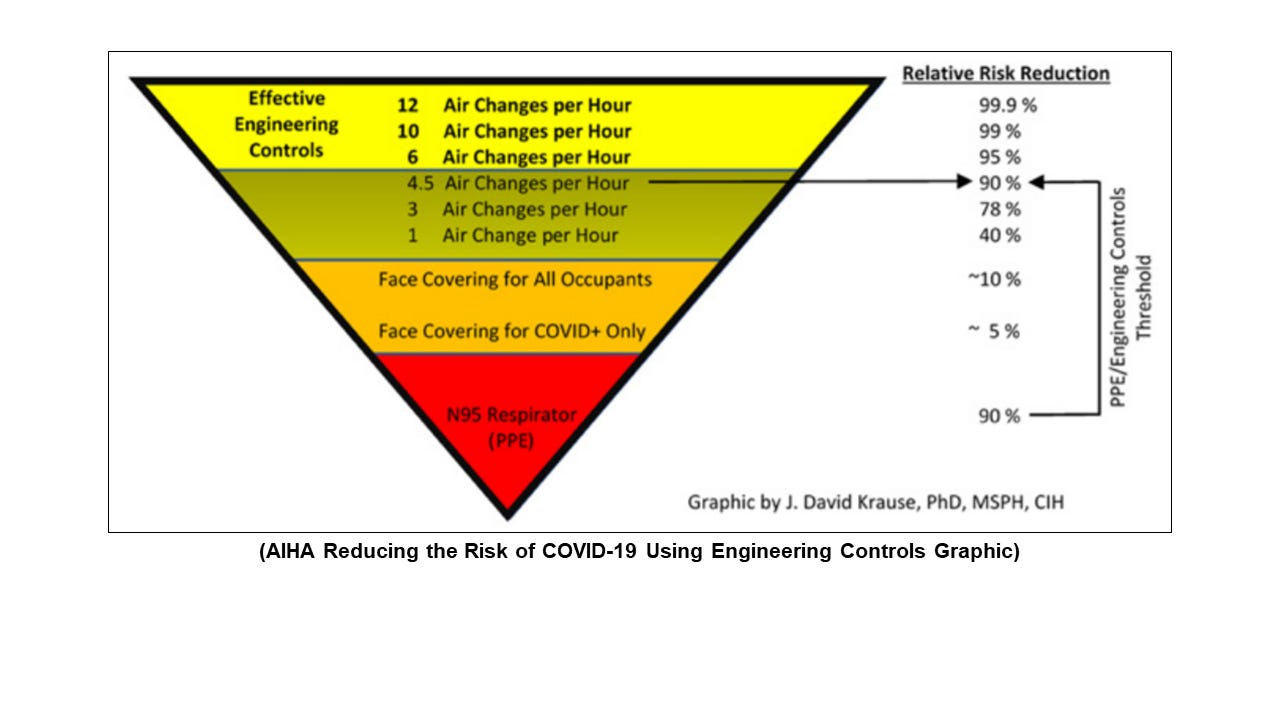
I do disagree with this graphic claiming that the N95 and face coverings actually provide relative risk reductions at the level claimed. This study was done in a medical setting with trained personnel in hygiene, sanitization, donning and doffing. This does not have relevance to the general public who does not have advanced or even proper training in these forms of PPE. In addition, the N95 does not provide proper protection for COVID-19 virus.
The “N” stands for non-oil resistant, which means it only have protective value in atmospheric conditions that excludes oil-based materials. The “95” means the filter efficacy is 95% for particles greater than 0.3 microns. Due to the material being non-oil resistant, it is made of weaker material than a standard reusable respirator and will degrade within two to four hours depending on the brand of N95 and how much moisture and heat the wearer is exposing the N95 to.
The N95 sucks, I would never recommend it as a protective measure to anyone outside of a medical setting. Medical facilities have state of the art HVAC systems that maintain proper indoor air quality and as mentioned before the personnel are trained for proper hygiene, sanitization, donning and doffing. An N95 would not survive an hour in a construction, mining, manufacturing, or maintenance settings and it would struggle to last two hours in a regular office or school setting. Essentially, the risks far outweigh any value provided by disposable masks or N95 respirators.
Okay, that’s my last mask/N95 rant…maybe. As you can tell, I’m not a supporter of either of those measures. What we must do in future pandemics is to hear from all aspects of scientists in this space. Remember we have two responses in any pandemic. The medical science response helps us understand the nature of the pathogen, which gives us an understanding of how to destroy it, how it enters the body, and how to formulate treatments for those that get exposed and sick.
The exposure mitigation response will take that valuable medical information and develop customized strategies in each setting to counter the pathogen. We will use the control options that are applicable to the occupied space and that have the capability to defeat the viral material. In addition, we will prioritize the control measures based on the Hierarchy of Controls and then train personnel in the control measures, their role within, and on which controls are better than others to ensure proper focus.
In a future article, I will share the general elements of the exposure mitigation plan we used to keep our clients safe, and their businesses open during the pandemic. Until next time, make it a safe day!
https://www.tyscienceguy.com/
Finally 😊🙏